Below is presented a case in which a new technique called MISOS1 (Minimally
Invasive Soft-Tissue and Osseous Stabilization) is used to stabilize a patient with
Eichenholtz I radiographic findings. Using this technique, deformity was addressed
proximal to distal as follows:
1) Ankle Equinus
2) Rearfoot Anatomic Restoration and
3) Beaming of Medial and Lateral Columns.
Dissection of the soft-tissue
envelope and associated angiosomes was kept to a minimum. All hardware was
delivered percutaneously. Beaming screws were placed intramedullary.
Intramedullary placement provided maximum stability from an engineering standpoint. After hardware delivery, a minimalist approach can be used to prepare
joints for fusion, employing trephine resection of articular surfaces and may be
augmented with the surgeon’s graft of choice.1
HPI: Patient S.A. is a 59 year-old female complaining of increase pain and swelling to
her left foot over the past year. The patient denies trauma. Serial radiographs
demonstrate progressive Charcot neuroarthropathic changes of the TMT complex
despite conservative care with CROW boot.
Review of Systems: Denies nausea, vomiting, fevers, chills, night sweats, calf pain,
and shortness of breath.
Past Medical History: Diabetes Mellitus Type-2, Dense Peripheral Neuropathy,
Charcot Neuroarthropathy, HTN, h/o DVT, and h/o hyperthyroidism.
Past Surgical History: C-section and Partial Thyroidectomy
Medications: Lantus and Humalog Insulin, Diovan, HCTZ, Calcium, and Lyrica
Allergies: Latex
SH: Full-time nurse, denies tobacco, ETOH, and illicit drugs.
PHYSICAL EXAM:
General: AVSS, AAOx3
Vascular: 2/4 DP&PT B/L, Increased edema LLE
Neurologic: 0/10 points discerned with monofilament
Dermatologic: Soft-tissue envelope is well maintained, no ulcers, no clinical signs of
infection.
Orthopedic: 5/5 MMT to all major LE muscle groups, profound decreased arch
height LLE upon weight bearing.
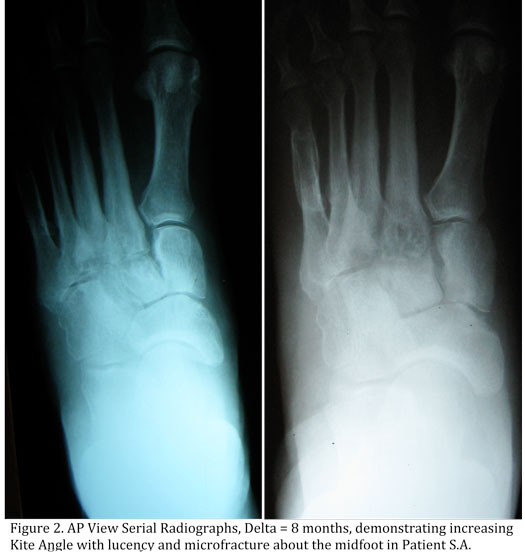
Radiographic: Serial plain films demonstrate increasing Meary Angle over time with
lucency and microfracture formation about the midfoot. CT of left foot demonstrates
microfracture and subchondral cysts throughout the midfoot. |
LAB DATA:
Electrolytes all within normal limits
WBC/Hgb/INR all within normal limits
HbA1c: 7.8.
ABIs & PVRs: 0.9 B/L with triphasic waveforms.
Arterial Duplex: All segments B/L LE are patent without evidence of disease.
In the case presented, Ankle Equinus is corrected via endoscopic gastrocnemius
recession, the Talo-calcaneal relationship is restored via subtalar arthroeresis, and
finally Medial and Lateral Columns are stabilized via intramedullary screws.
Post-operatively patient S.A. was placed in a large-well-padded-limb-preservation
dressing with posterior, medial, lateral, and anterior splints, kept NWB LLE for three
months with wheelchair and walker, and was prophylaxed for DVT with enoxaparin.
At six months post-operatively, patient S.A. has returned to full-time nursing
without restriction, ambulating in a custom-molded diabetic shoe.
PHYSICAL EXAM: Upon physical exam, the patient is noted to be neurovascularly intact with pedal pulses palpable and graded +2/4 bilaterally. The patient demonstrates a bilateral metatarsus adductus deformity noted which is worse on the left than the right. (Figs.2, A-B below) This deformity is noted to be reducible with manipulation. There is no equinus noted. Muscle strength appears to be within normal limits, and the patient does not demonstrate a Babinski reflex. The patient demonstrates no knee or hip abnormalities.
Radiographs and images: Please be sure to follow our eTalk discusion on this intriguing case study, following the radiographs and photographs.
Reference:
1Thomas S. Roukis, Minimally Invasive SoftTissue
and Osseous Stabilization
(MISOS) Technique for Midfoot and Hindfoot Deformities, Clinics in Podiatric
Medicine and Surgery, Volume 25, Issue 4, Surgical Reconstruction of the High-Risk
Patient, October 2008, Pages 655-680, ISSN 0891-8422,
DOI: 10.1016/j.cpm.2008.05.005.
We'll see you next week. Best wishes!
|






































.jpg)

















