We have a very special guest editor today, Jeffrey Siegel, DPM, FACFAS. Dr. Siegel completed his undergraduate training at the University of California, after spending four years as a Hospital Corpsman and Paramedic in the US Navy in San Diego. He holds a Bachelors of Science degree in Biology with minors in Psychology and Organic Chemistry. Graduating with top honors from The California College of Podiatric Medicine in 1990, Dr. Siegel completed his internship and surgical residency at Kaiser Permanente Medical Center in Santa Clara, California. Dr. Siegel acquired advanced training in both pediatric and adult reconstructive surgery, foot and ankle trauma, and diabetic wound care/limb salvage strategies. He spent time in Baltimore, MD at the Mt. Sinai Hospital/Rubin Institute and Kurgan Russia studying advanced deformity correction using Ilizarov techniques. Dr. Siegel has held academic appointments at Stanford University, UCSF School of Medicine, The California College of Podiatric Medicine and The University of Osteopathic Medicine and Surgery in Des Moines Iowa.
Noteworthy, Dr. Siegel is among a small group of podiatric physicians nationally that have earned double Board Certification in Foot and Reconstructive Rearfoot/Ankle Surgery and Podiatric Orthopedics and Primary Podiatric Medicine. Dr. Siegel is a Diplomate of the American Board of Podiatric Surgery and a Fellow of the American College of Foot and Ankle Surgery. Currently, he is in his 20th year of practice and is an Adjunct Assistant Professor of Surgery and Medicine the Temple University of Podiatric Medicine. Dr. Siegel specializes in the treatment of athletic injuries, pediatric disorders, diabetic infections, complex wound care and limb salvage. Along with his partner Dr. Charles Morelli from Ney York, Dr. Siegel travels to Nicaragua every year to participate in a humanitarian medial mission trip. Last year, the pair operated on 30 patients in four days. Dr. Siegel is married with two grown boys and two teenage stepdaughters. Hobbies include all things family oriented, gourmet cooking and of course eating. However, his biggest passion is nutrition, fitness and amateur bodybuilding promoting a healthy mental, physical and spiritual lifestyle.
—Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]
Charcot Neuroarthropathy
Case Study, Part 1
Jeffrey Siegel, DPM, FACFAS, DABPO
Adjunct Assistant Professor, Depts. Of Medicine and Surgery, TUSPM
A 78 year old WF presents to the office for a second opinion regarding her severely deformed right foot. Mrs. B states that 6 months ago she was diagnosed with a diabetic ulcer on the medial arch that required two procedures to close. Patient denied ulcerations on the bottom of her foot. Over this time period, her foot had become progressively deformed, swollen, red and painful when she walks. Mrs. B stated that "I was told that I have Charcot foot and that I have to live with it because nothing can be done." Past treatment included: Non-weight bearing and custom molded shoes. Her BS ranges from 80 - 160. States that she was diagnosed with diabetes just two years ago, but has had numb feet for years. Mrs. B. uses a cane normally and her post-operative goal is to be able to perform her normal activities of daily living.
Allergies: NKDA.
Medication History: Actos, Aspirin, Caltrate 600 with D, Carvedilol, Centrum Silver, Ferrous gluconate, Fish Oil, Levothyroxine, Lisinopril, Magnesium carbonate, Neurontin, Warfarin.
Past Medical History: Cardiovascular Hx: (+) hypertension (HBP), (+) pacemaker.
Musculoskeletal Hx: (+) arthritis conditions.
Hematologic / Lymphatic Hx: (+) anemia.
Endocrine Hx: NIDDM x 2 yrs.
Past Surgical History: Insertion of dual chamber pacemaker; right 2nd toe amputation and debridement right arch (medial cuneiform) and a second debridement for wound dehiscence.
Social History: Patient denies smoking, alcohol abuse, illicit drug use, and STDs.
Family History: Unremarkable.
Review of Systems: Unremarkable with exception of chief complaint and all other systems are negative.
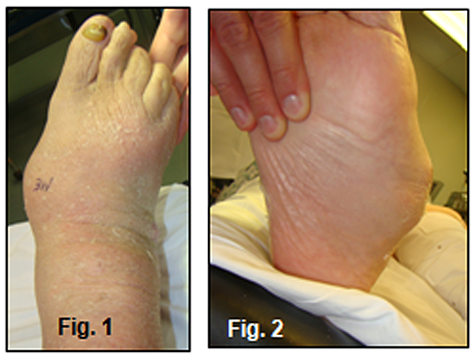
Physical Exam: Examination revealed evidence of a Lisfranc’s deformity with complete collapse of the foot yielding a very prominent medial midfoot and rigid, laterally deviated forefoot (Figure 1,2).
There is a well healed incision over the medial cuneiform (Figure 3).
The foot has mild edema and erythema and there is no lymphangitis, adenopathy or open lesions. There is, however, an area of fluctuance over the dorsolateral midfoot that when aspirated, yielded 5 cc's of an opaque, blood tinged fluid (Sent for C & S).
Vascular: DP/PT pulses are 2/4, bilateral. Capillary fill time is immediate. No contralateral lower-extremity edema is noted and varicosities were not observed.
Derm: Skin temperature of lower extremities warm to warm proximal to distal. Skin inspection was otherwise unremarkable. Mycotic changes noted in the nails 1-5 bilateral.
Neuro: The 5.07 monofilament test was performed and there was profound evidence of loss of protective sensation. Touch, pin, vibratory, and proprioception sensations were abnormal. Deep tendon reflexes diminished.
Ortho: Examination of the patient’s ankle joint dorsiflexion reveals limitation of dorsiflexion of foot relative to leg with knee extended AND flexed consistent with gastroc-soleal equinus deformity. There is loss of stability of the foot with significant hypermobility and excessive dorsiflexion and abduction of the midfoot. Crepitus noted with ROM consistent with an acute vs. chronic Charcot deformity. Muscle strength 5/5 for all groups tested. Muscle tone normal. Mild genu valgus B/L. Inspection and palpation of bones, joints, and muscles otherwise unremarkable.
Diagnostic Studies: Non-weight bearing plain films and 3D CAT Scans: Evidence of a displaced, comminuted fracture-dislocation of the Lisfranc joint w/collapse of the medial cuneiform and severe lateral deviation of the forefoot (Figure 4-6). Hypertrophic degenerative changes are present in the midfoot. The pre-op lateral view is partial weight bearing which explains the normal appearing talocalcaneal relationship vs. post-op weight bearing views. There is some rounding and sclerosis at the 1st TMT joint. Osteolytic changes are seen in the body of the cuboid consistent with acute Osteomyelitis (Fig. 4). CAT Scan evidence plantar and medial displacement of the medial cuneiform and collapse of the cuboid (Figure 7-8). Hindfoot and ankle views are WNL.
| Part Two of this case study to be presented in next week's Practice Perfect |
| Look for Part 2 next week, where we will present exactly how Dr. Siegel assessed the findings above and treated this patient — you will be surprised. In the meantime, please take a few moments to share your thoughts in our eTalk forum, on how YOU might plan to treat this patient. |
|

Keep writing in with your thoughts and comments. Better yet, post them in our eTalk forum. Best wishes.
Frykberg PRESENTs 4th Oration to Diabetic Foot Society of India |
Robert G. Frykberg, DPM, MPH, PRESENT Editor for Diabetic Limb Salvage, just returned from his 4th trip to India to present his 2010 annual Diabetic Foot Society of India (DFSI) Oration in Bangalore. He was asked to present his overview on the “Diabetic Charcot Foot 2010: Surgical Indications”. The DFSI is that nations’ largest society dealing with the study of diabetic foot complications, including medical, surgical, and biomechanical management. This year’s meeting was wide ranging in presented topics, including wound pathophysiology and appropriate debridement techniques, diabetic foot infections and microbiology, surgical approaches to the diabetic foot, the role of angiosomes in proper operative planning for flaps, as well as numerous topics on biomechanical considerations and wound treatments. Other International faculty included Christopher Attinger, MD (USA), Giacomo Clerici, MD (Italy), and Ralf Lobmann, MD (Germany). They were joined by 300 Indian physicians and nurses, including the DFSI Executive Planning Committee: Kal Suresh, MD, Arun Bal, MD, and Dr. G. Goyal, MD. |
|
|
Get a steady stream of all the NEW PRESENT Podiatry
eLearning by becoming our Facebook Fan.
Effective eLearning and a Colleague Network await you. |
 |
|