| |
 Ryan Fitzgerald, DPM
Ryan Fitzgerald, DPM
PRESENT RI Associate Editor
Hess Orthopedics &
Sports Medicine
Harrisonburg, Virginia
|
Case Conclusion:
A 44-y/o Male with a Neglected
Achilles
Tendon Rupture
There have been some excellent responses regarding this challenging case via the eTalk thread on this topic at PRESENT Podiatry!
If you did not get a chance to read part 1 of this case study, or would just like to review, you can follow this link to read the eZine.
As many of you noted, the MRI images demonstrated significant retraction of the tendon –largely due to the delay in seeking treatment. Considering this patient’s age and mobility status, the decision was made to bring the patient to the operating room for surgical correction of this deformity.
Following surgical debridement of the free ends of the tendon, there was significant gapping noted (fig.1). Considering this significant loss of tendon integrity, the decision was made to perform a gastrocnemius recession to lengthen the posterior structures and reduce the overall gap. Following this, cadaveric achilles tendon graft was utilized to bridge the remaining gap between the free proximal and distal achilles tendon ends (fig. 2).
|
|
| Figure 1:Following debridement, the patient demonstrated a significant gapping between tendon ends. |
|
|
|
| Figure 2: Cadaveric graft was utilized to bridge the free achilles ends. |
|
Following placement of the achilles tendon graft (fig. 3), an Integra Inforce™ (Integra LifeScience, Plainsboro, NJ) collagen graft was placed to provide further stability at the repair site (figure 4a, b).
|
|
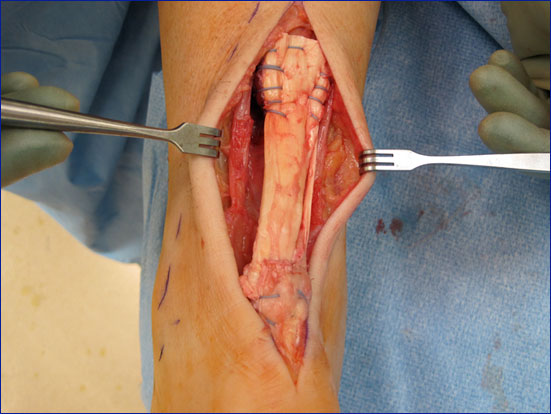
Figure 3: The cadaveric tendon graft was sutured into place utilizing fiber wire. The plantaris tendon was incorporated into the repair to provide additional stability.
|
|
|
|
| Figure 4a: The Inforce collagen graft was placed prior suturing the proximal portion of the cadevaric graft. |
|
|
|
| Figure 4b: The Inforce™ graft was sutured in place following placement of the proximal portions of the cadaveric achilles tendon graft. |
|
The tendon graft was placed with the foot in slight plantar flexion, and the patient was placed into a modified Robert Jone’s dressing post operatively. Following suture removal at fourteen days, the patient was placed into a short leg, non-weight bearing cast. He was then kept immobilized for approximately eight weeks. Following this, the patient was placed into a removable cam walker (RCW), and allowed to progressively weight bear. It was at this time that physical therapy was initiated to improve both strength and range of motion.
The patient is currently six months post-op and has returned to full activity without incident and is currently training for a triathalon.
We love hearing from you. I encourage all of our readers to participate in the online forum in the etalk thread on this topic, and post your thoughts, pearls, and perspectives regarding this (or any other) interesting case.

Get a steady stream of all the NEW PRESENT Podiatry
eLearning by becoming our Facebook Fan.
Effective eLearning and a Colleague Network await you. |
 |



















.jpg)


















