The real-world healing of complex, refractory wounds can be problematic. Wounds with undermining, poor tissue generation, and resistant microbial barriers are common occurrences and present special challenges in wound care, especially among high-risk, debilitated patients. Research has revealed that delayed healing may be due to a self-sustaining biofilm matrix on the wound bed which is present in over 90% of chronic wounds. Unchecked, biofilm impairs wound healing through induced chronic inflammation, leads to biofilm-based infection, and protects the bacteria within the matrix from even the most robust external attack. Expert opinion now supports a new perspective toward biofilm directed interventions that disrupts the protective biofilm matrix. Use of biofilm disrupting technology is crucial as an early adjunctive treatment option for chronic wounds.
OBJECTIVE:
This is a case series report of the author’s experience with the use of a biofilm disrupting gel on complex wounds that were considered hopeless and placed in palliative care. Wounds exhibited intractable drainage, odor, and undermining, with failed prior treatments that severely affected quality of life.
MATERIALS AND METHODS:
Patients were selected who were unresponsive to standard wound care (no reduction in wound surface area for >4 weeks), had undermining or tunnels, were not candidates for aggressive debridement, had failed antimicrobial dressings (exhibited copious, green or malodorous drainage despite various dressing products), had inadequate granulation tissue, and were not candidates for an advanced therapeutic. The biofilm disrupting gel was provided with various dressings as well as any appropriate off loading, and nutritional supplementation.
RESULTS:
Patients applied the biofilm disrupting gel at regular dressing changes ranging from daily to three times per week and were followed at regular intervals (weekly and then later bimonthly).
DISCUSSION/CONCLUSION:
True wound healing is often hard to quantify with numbers alone. How can you measure a patient’s quality of life, the hope of healing where there was no healing, alleviating the embarrassing effects of odor? How do you tell debilitated patients they have to lay in one spot furthering their confinement? With this patient series, the opportunistic persona of biofilm presents more than a superficial, invisible barrier to wound healing. For patients thought to be hopeless, out of options, and palliative, the use of BlastXTM, a member of the XbioTM family of products, has affirmed that when opportunities to improve care present, they should be considered for EVERY patient.
Despite having failed numerous prior therapies, patients on the biofilm disrupting gel resolved undermining, had a decrease in slough, an increase in granulation tissue and in some cases, epithelialization. Biofilm disruption technology promises to remove one of the greatest barriers to healing.
Case 1
Severe inoperable wound from irradiated cancer site
STATUS = HEALED ABSCESS, RESOLVING WOUND
This is a right breast auto amputation. Abscess under the rib (left circle), draining spontaneous abscess below. Local disease eradicated by XRT – currently no active cancer in the wound bed. The patient was still working but dealing with heavily exudative wounds and odor due to polymicrobial colonization. She was facing extensive plastic surgery for possible closure, but team was not sure she would survive. The lesion on her chest has been present since about September 2016. She recovered from pathological fractures of the right arm and right leg due to metastasis and was doing well on maintenance immunotherapy. It was assumed that, despite her grim long-term prognosis, she may live years. On 12/19/17 she complained that a deep area on the right anterior chest wall was very painful. Visible pleural movement was noted at the base of the wound through what appeared to be an erosion of a rib although the patient was not systemically ill. Some days later, pus began to drain through the opening in the chest wall and the pain dramatically improved. She was seen by plastics but given the fact that covering the defect would be unlikely after a wide debridement, a conservative plan was recommended. Local debridement was avoided because the area was hypoxic due to radiation tissue damage. DNA assay revealed a variety of non-pathogenic facultative organisms. Traditional culture showed enterococcus. She was placed on Vitamin D, Zinc and L-arginine.
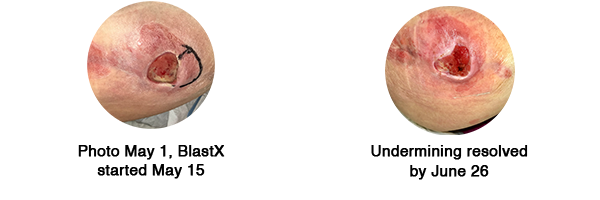
Case 2
Severe undermining
STATUS = RESOLVED
Young male patient with Cerebral Palsy and psoriasis for years, developed ischial pressure ulcer during hospitalization for pneumonia that had been non-healing for months, BlastX started on May 15, undermining resolved, with healthier appearing wound bed in five weeks.
Regards,
Caroline Fife, MD
Medical Director
Wound Care Center
CHI St. Luke's The Woodlands Hospital
###
For more information on 3M Wound Care Solutions, please visit www.3m.com/woundcare





Comments
There are 0 comments for this article